ARTHRITIS & YOUR KNEE
Arthritis of the knee joint (usually osteoarthritis) is basically wear and tear of the joint. The knee can wear out because of age or because of a previous injury which accelerates wearing of the knee joint.
Pain may have been experienced in one or both knees for some time, with limited movement when squatting or walking up and down stairs. There may also be a “crunching" of the knee which can be heard and felt when bending the knee.
On examination of the knee, Dr Wood may request an X-ray to confirm the diagnosis by viewing the joint space, the gap between the thigh bone (femur) and shin bone (tibia). This gap is usually made up of meniscus and articular cartilage (similar to the shiny white gristle seen on the joint. Articular cartilage does not show up on X-ray and thus appears as a gap.
If this articular cartilage is worn out by a previous injury or by wear and tear, the gap or joint space narrows, sometimes to the degree where bone rubs on bone and becomes very painful, causing crunching of the knee.
The options for treating arthritis depend on a number of factors:
- Age
- Severity of arthritis
- Weight
- General health
- Amount of pain – at rest and walking
- Lifestyle
These factors also help Dr Wood decide on the treatment of the arthritic knee - conservative treatment or surgery.
Conservative treatment is usually chosen for younger people (30 to 60 years) when the disease is mild to moderate and little pain is experienced. This may include anti inflammatories, physiotherapy and a change in lifestyle ie avoiding all twisting sports or change of job. Some people can go on for many years being treated conservatively and some deteriorate rapidly to severe pain which may require surgery.
Surgery may be recommended for older patients who have severe pain and arthritic changes on X-ray.
For those people who are still young (40 to 60 years) a high tibial osteotomy may be necessary to alleviate the pain and grinding of the joint. This operation is 70% successful and thorough discussion with Dr Wood is necessary before proceeding to surgery.
A successful high tibial osteotomy is especially good for those people who wish to return to an active lifestyle with little restriction on activities.
For the more senior patients (60+ years) a total knee replacement may be necessary when pain in their knee is constant and prevents them from enjoying a good quality of life eg walking to the shops or playing nine holes of golf. If a patient has pain at rest and at night preventing sleep it is probably time for a total knee replacement.
It is important to emphasise that a total knee replacement is only performed to relieve pain. It will not enable you to kneel, play netball, touch football, ballet or any twisting type activities or sports. It will help improve the quality of life so that you can walk to the shops or play golf.
Sometimes a knee replacement will be performed on a younger person (40+ years) if their arthritic knee pain is severe and their quality of life is poor.
This operation is 95% successful but with a recovery time of six months. Thorough discussion with Dr Wood involving the potential complications of this operation is necessary. Only when you are prepared to accept the risks of surgery should you consider having this performed.
The chance of developing arthritis because of arthroscopic surgery for a torn meniscus?
The chances of developing post traumatic arthritis is not because of the surgery but because of the injuries. The chance of arthritis is 100% after about 7 – 10 years, if the medial meniscus tore. The chance of arthritis is 100% after about 4 – 5 years, if the lateral meniscus tore.
How bad the arthritis will be depends upon the patient's body physiology and the other damage done to the knee at the time of the injury when the meniscus tore. However, if the torn meniscus is allowed to remain in the knee the amount of arthritis will usually be greater, more painful, and will develop much faster than if the torn part of the meniscus is removed.
TOTAL KNEE REPLACEMENT
INFORMATION
The time has come, possibly after many years of pain and discomfort, to replace your worn knee joint.
It is important to understand a few things concerning your knee. The operation is performed for one reason only – pain relief. Afterwards you will not be able to kneel, squat, crawl, climb ladders, play tennis, jog or do any other twisting type sports. It will help you walk eighteen holes of golf without pain, or walk to your local shops.
Recovery from your operation will take some time – five to seven days in hospital for a single joint replacement and then recuperation for a further week in a rehabilitation hospital. This depends on your post operative recovery and your situation at home - if you have someone who can help look after you.
No two knees are the same and everyone recovers at a different rate for a number of different reasons (eg fitness, other affected joints and medical problems). If both knees are operated on then one will recover more quickly than the other.
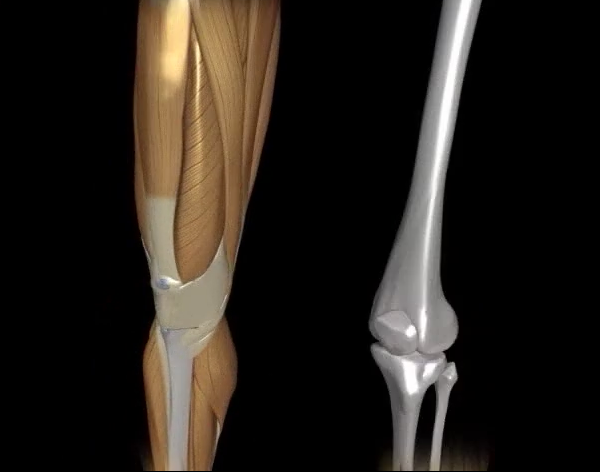
THE KNEE
How does the knee work?
The knee joint functions like a hinge at the junction of two bones, the femur (thigh bone) and tibia (shin bone). The ends of the bones are covered with a thick cushion of hard white cartilage. There is only one coating of this cartilage in a lifetime and if it is damaged or worn away, the underlying bones rub together, producing the pain and inflammation typical of arthritis.
What is arthritis?
Arthritis is inflammation of a joint causing pain, swelling, stiffness, instability and often deformity. Severe arthritis interferes with activities and limits lifestyle.
What causes arthritis in the knee?
Osteoarthritis or Degenerative Joint Disease. The most common type of arthritis. Osteoarthritis is also known as “wear and tear arthritis" since the cartilage simply wears out. When cartilage wears away, bone rubs on bone causing severe pain and disability. The most frequent reason for osteoarthritis is genetic, since the durability of each individual's cartilage is based on genetics.
Trauma can also lead to osteoarthritis. A bad fall or blow to the knee can injure the joint. If the injury does not heal properly, extra force may be placed on the joint, which over time can cause the cartilage to wear away.
Inflammatory Arthritis. Swelling and heat (inflammation) of the joint lining causes a release of enzymes which soften and eventually destroy the cartilage. Rheumatoid arthritis, Lupus and psoriatic arthritis are examples.
How can a doctor diagnose arthritis?
Doctors diagnose arthritis with a medical history, physical examination and X-rays of the knee.
What is a total knee replacement?
When the cartilage has worn away, an artificial knee (called a prosthesis) can take its place. The surgery to implant the prosthesis is termed a total knee replacement. Only the surface of the joint is removed. The arthritic ends of the bones are shaved off and replaced with new metal and plastic surfaces. The knee replacement recreates some, but not all, knee functions.
Who should have a total knee replacement?
The most common reason for a total knee replacement is severe arthritic pain. Pain cannot be measured, and the degree of pain sufficient to warrant surgery should be decided by the patient and doctor together. Painful and arthritic knees often become unstable and untrustworthy, causing falls and other injuries. The patient's independence is compromised and the quality of their life will decrease.
What are the benefits of total knee replacement?
The goal of a total knee replacement is to relieve pain. It may also help to restore motion and straighten the limb.
What is the short term outlook?
Most patients can stand the second day after surgery and begin exercising that day. With the support of walkers or crutches, patients can walk with confidence, climb stairs and ride in a car by the time they leave hospital. Physiotherapy and motion exercises help recovery and should continue for months. Some swelling, aching and numbing are normal during this time. Most patients are up and about within six weeks.
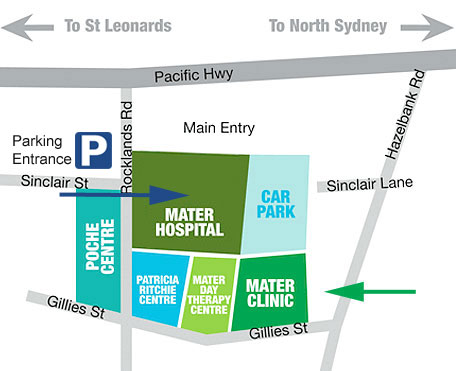
Surgery
Surgery will be performed at the Mater Private Hospital on a Monday afternoon. Hospital staff will admit and prepare you for surgery. The Anaesthetist will see you prior to surgery. Please advise the Anaesthetist of any medications you are taking.
There are two parts to the surgery:
Firstly: the femur is cut and a titanium femoral prosthesis is put in place.
Secondly: the tibia is cut and a titanium tibial plate is put in place with four screws. A plastic articulating cartilage is placed inbetween the femur and tibia to act as a shock absorber, as well as a barrier between the metal. If the plastic wears out it is easily replaced.
In some knees the patella (knee cap) will also be resurfaced.
A drain will be in place for a couple of days and the wound closed with dissolving sutures or skin clips. Your leg will be wrapped with cotton wool and crepe bandages.
If you had an epidural anaesthetic in your back this will help with pain relief post operatively. If not, recovery and ward staff will offer pain killers.
You will commence physiotherapy (usually the day following surgery) to help you mobilise as soon as possible.
Risks of surgery:
The anaesthetic can cause problems. Discuss any concerns with your Anaesthetist.
Blood clots (DVTs) can form following surgery. You will be given blood thinners in hospital and checked about the seventh day for blood clots with an ultrasound machine.
Infection is the most difficult problem to treat and occurs in about 1% of patients.
You will be given antibiotics in hospital.
If you take Aspirin or Warfarin please advise your doctor as you will cease taking it about ten days prior to surgery.
Post operatively
Your recovery depends on you. Remember to take it easy and not overdo things during your immediate post operative period.
The healing process for a total knee replacement can be very slow. It can take up to six months to fully recover – depending on your circumstances it may be more or less than this time.
It is important not to compare yourself with others who have had this surgery as each individual's recovery is different.
Knee replacements are painful for at least three months and some longer. You will never get full bend back or normal function.